Despite CT is obviously superior to MR in diagnosis of craniocervical junctional bone anomalies,
these anomalies are recognized by MR as well [7].
In this exhibition,
CT and MR evaluation were done by using normal line and angle values.
Herein we present CT and MR images of CCJ anomalies for each case.
We used classification of Chen and Liu.
This is an educational exhibit.
No scientific data will be presented.
Congenital Anomalies
1.Occipital bone
1.1 Platybasia
Platybasia identified it as an X-ray finding.
The simplest definition is to determine the skull base flattened.
Manifested by enlarged Welcher basal angle [5].
Platybasia may be asymptomatic if there isn't accompanying basilar invagination and any other anomalies of skull base.
The most common accompanying anomaly when platybasia is detected is basilar invagination [3]. Fig. 5
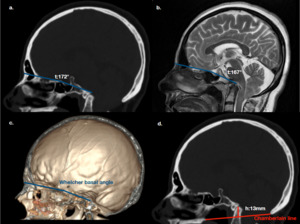
Fig. 5: Platybasia: (a.) Mid-sagittal reformatted CT image evaluated with Welcher basal angle (It is meaningful in terms of platybasia above 140 °). (b.) Sagittal T2W MR image; flattened skull base, enlarged Welcher basal angle. (c.) Volume rendering 3D image; nasion-tuberculum sellae line and tuberculum sellae-clivus line (Tuberculum sellae-basion). (d.) Mid-sagittal reformatted CT image; basilar invagination.
1.2 Basioccipital hypoplasia
Basiocciput develops from the first and second occipital sclerotome and forms posterior inferior parts of the clivus.
Platybasia is not observed in most basilar invagination patients,
so the Welcher basal angle is normal.
The clivus canal angle has narrowed,
which can cause severe craniomedullary junction pressure.
Compression is best demonstrated by mid-sagittal MR evaluation [3][4][8]. Fig. 6 Fig. 7
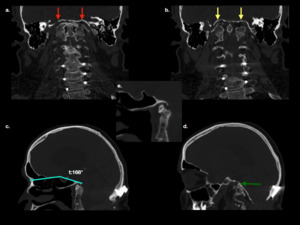
Fig. 6: Basioccipital hypoplasia: Operated cervical stabilization patient. (a.) Coronal reformatted cervical CT image, red arrows point to clivus. (b.) Coronal reformatted cervical CT image, yellow arrows point to condyles. (c.) Mid-sagittal reformatted brain CT image; flattened skull base, enlarged Welcher basal angle. (d.) Left lateral sagittal reformatted brain CT image; very distinct condyle hypoplasia green arrow point to left occipital condyle. (e.) Mid-sagittal reformatted brain CT image; clivus is almost never developed.
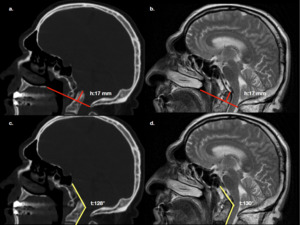
Fig. 7: Basioccipital hypoplasia: (a.) Mid-sagittal reformatted brain CT image, (b.) Mid-sagittal T2W MR image; odontoid process above 17 mm on the Chamberlain line. (Basilar invagination) (c.) Mid-sagittal reformatted brain CT image, (d.) Mid-sagittal T2W MR image; clivus canal angle narrowed and spinal canal stenosis.
1.3 Condylar hypoplasia
Occipital condyles originate from the third sclerotome.
From the same embryological structures,
the jugular tubercles also differentiate [3][9].
In the hypoplasia of the occipital condyles,
the skull base is flattened and medialized.
The narrowing of the clivus canal angle in mid sagittal reformatted images is significant for diagnosis,
but in the coronal reformatted images,
the increase of the atlanto-occipital joint axis and the flattening of the joint are the most important radiological findings. Fig. 8 Fig. 9
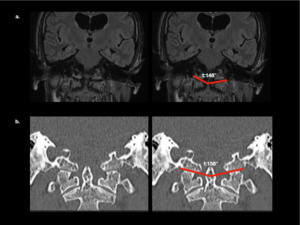
Fig. 8: Condylar hypoplasia: (a.) Mid sagittal T2 FLAIR MR image, (b.) Coronal reformatted brain CT image of the same patient, widening of the atlanto-occipital joint axis angle. The complaint from the patient was headache. Hydrocephalus was detected at imaging and clinically confirmed.
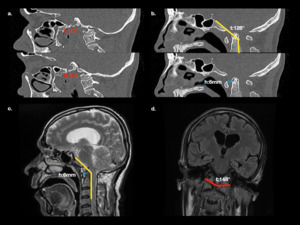
Fig. 9: Condylar hypoplasia: (a.b.) Mid-sagittal reformatted brain CT images;Condylar hypoplasia and increased anterior atlanto-dental interval, horizontal distance between the anterior arch of the atlas and the dens of the axis, atlanto-axial dislocation is defined as AADI greater than 3 mm in adults. (c.) Mid sagittal T2W MR image; clivus-canal angle is abnormal. Narrowed clivus canal angle should be stimulating in terms of condylar hypoplasia. (d.) Coronal T1W MR image; widening of the atlanto-occipital joint axis angle.
1.4 Condylar dysplasia
Condylus tertius
Anterior tubercle of clivus derivates from fourth occipital sclerotome also known as proatlas [10].
Proatlas persistence or fails to integrate,
well corticated oval shaped ossified remnant may be present at the distal end of the clivus,
named the condylus tertius or third occipital condyle [9].
Third occipital condyles may be associated with cervical canal stenosis, hypoplasia of the dens [10].
Condylus tertius may articulated or pseudo articulated with the clivus,
anterior arch of atlas,
or dens axis [3].
There is an increased prevalence of os odontoideum associated with condylus tertius [5]. Fig. 10 Fig.
11
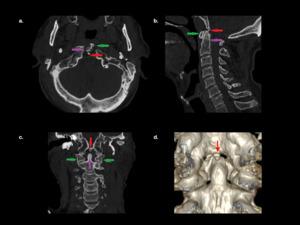
Fig. 10: Condylus Tertius (a.) Axial cervical CT image (b.) Midsagittal reformatted cervical CT image (c.) Coronal reformatted cervical CT image. Green arrow:C1(Atlas), Purple arrow: Odontoid process, Red arrow: Condylus Tertius. Proatlas persists or fails to integrate clivus, an ossified well corticated remnant present at the distal end of the clivus. (d.) 3D volume rendering image posterior view
2.
Atlas
2.1 Atlas assimilation
Atlas derivates from proatlas and first spinal cervical sclerotome.
During the development of these embryological structures,
there is no segmentation or failure,
resulting in partial or complete assimilation.
This non-segmentation,
also known as occipitalization of the atlas.
The assimilation may be limited to the anterior arch,
the posterior arch,
the lateral masses,
or exist in combination.
Atlas assimilation can be unilateral or bilateral.
Unilateral atlas assimilation caused torticollis in children [9].
New anatomical studies indicate that atlas assimilation is more prevalent than thought [11].
Atlas assimilation can predispose to atlanto-axial dislocation [12]. Fig. 11 Fig. 12 Fig. 13
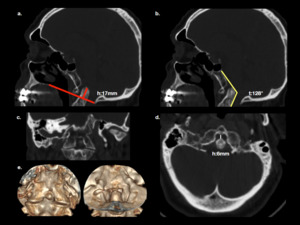
Fig. 11: Atlas assimilation: (a.) Mid sagittal reformatted brain CT image; basilar invagination. (b.) Mid sagittal CT image; clivus canal angle is abnormal and angulated odontoid process. (c.) Coronal reformatted CT image; no junction between occiput and atlas, atlas assimilation. (d.) İncreased atlanto-dental interval; Atlanto-axial dislocation. (e.) Volume rendering 3D image; anterior and posterior view.
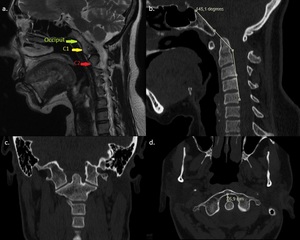
Fig. 12: Atlas assimilation: (a.) Sagittal T2W cervical MR represents assimilated bone narrow. (b.) Mid sagittal reformatted CT image: mild narrowed clivus canal angle and angulated odontoid process. (c.) Axial CT image, no joint between occiput and atlas; atlas assimilation. (d.) Coronal reformatted CT image, increased atlanto-dental interval; atlanto-axial dislocation.
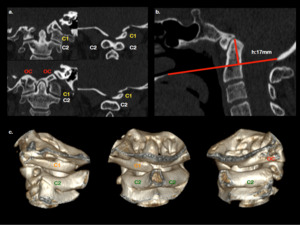
Fig. 13: Aplasia and hypoplasia of the atlas: (a.) Coronal reformatted CT images; 1.Rudimental left lateral mass of atlas articulates with hypoplastic occipital condyle. 2.Left transverse process of Atlas(C1) is present but right transverse process is not. 3.Atlas(C1) right posterior arch aplasia. 4.Atlas(C1) Posterior arch rashishizis. (b.) Mid sagittal reformatted CT image; basilar invagination. (c.) 3D volume rendering images; 1.Left oblique 2.Posterior 3.Rigth oblique
2.2 Atlas arch anomaly
The lateral atlas masses and superior portion of the posterior atlas arch are formed by the caudal division of the neural arch of the proatlas,
while the first spinal sclerotome forms the atlas(C1).
Most atlas anomalies are posterior arch anomalies,
probably due to a developmental failure of chondrogenesis.
The most common atlas arch anomaly is posterior arch rachischisis.
Anterior arch rachischisis is rare,
when it occurs with posterior arch rachischisis,
called split atlas [13].
In split atlas,
the anterior arches are hypertrophied.
Fig. 14 Fig. 15
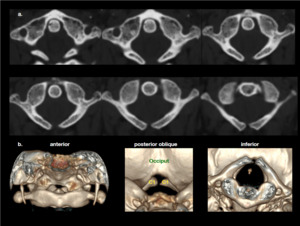
Fig. 14: Atlas arch anomaly: (a.) Serial axial CT images of atlas (C1); posterior arch rachischisis. (b.) Volume rendering 3D image; posterior oblique and inferior images demonstrates posterior arch rachischisis.
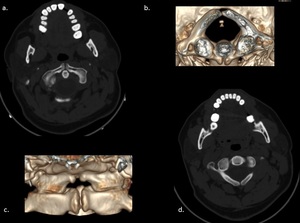
Fig. 15: Atlas arch anomaly: (a.) Axial CT image; anterior arch rachischisis. (b.) Volume rendering 3D image; inferior view of split atlas. (c.) Volume rendering 3D image; anterior view of split atlas. (d.) Axial CT image; posterior arch rachischisis.
2.3 Aplasia and hypoplasia of the atlas
It usually accompanies rachischisis and arch anomalies.
Aplasia and hypoplasia may be partial or complete,
may be unilateral or bilateral.
The incidence of Klippel-Feil anomalies in the C1-C2 vertebral corpus has increased.
Condyle hypoplasia,
platybasia,
basilar invagination,
compensatory cervical scoliosis may be accompanied. Fig. 22
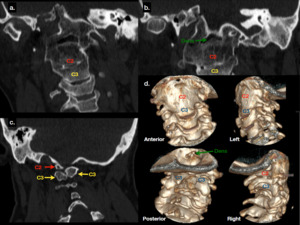
Fig. 22: Aplasia of the atlas and Klippel-Feil Anomaly: (a.) Coronal reformatted CT image; Axis(C2) articulates with hypoplastic occipital condyles. (b.) Coronal reformatted CT image; Right occipital condyle is more hypoplastic than left one. In the Axis(C2) anterior mass, the dens are fused and hypoplastic (c.) Coronal reformatted CT image; C2 left posterior arch aplasictic and C3 posterior arch rachischisis (d.) Volume rendering 3D images; Condylar Hypoplasia, Aplasia of the atlas(C1), C2 and C3 fusion, C2-C3 posterior arch rachischisis.
3.
Axis and odontoid process
3.1 Aplasia or hypoplasia of the dens
Dens aplasia is very rare.
Excavation defect may be seen in axis anterior corpus below the level of articular process.
The height of the dens in the dens hypoplasia is lower than the height of the atlanto-occipital joint.
Dens bicornuate results from atypical distal ossification leading to failure of development of apical dental segment [14]. Fig. 16
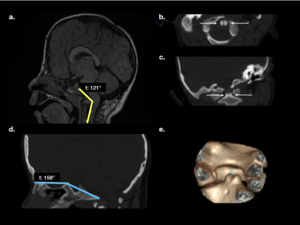
Fig. 16: Hypoplasia of dens: (a.) Sagittal T2W MR image; enlarged clivus canal angle. (b.) Axial CT image; represents hypoplastic dens bicornuate. (c.) Coronal reformatted CT image; Platybasia. (d.) Mid sagittal reformatted CT image; hypoplastic dens bicornuate is a very rare malformation. (White arrows hypoplastic dens bicornuate)(e.) 3D volume rendering image; posterior oblique view
3.2 Persistent ossiculum terminale
Os terminale and the apical ligament develops from proatlas central portion.
Dens develops from the first spinal sclerotoma.
The persistent ossiculum terminale results from failure of fusion of the proatlas to the rest of the odontoid process.
In some rare cases,
it can be seen in multiple and different shapes.
Odontoid is always normal height in this anomaly [15][16].
Fig. 17
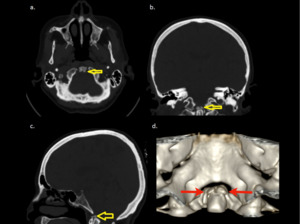
Fig. 17: (a.) Axial CT image(yellow arrow); (b.) Coronal reformatted CT image(yellow arrow); (c.) Mid sagittal reformatted image(yellow arrow) (d.) Volume rendering 3D image(red arrows) posterior view; well-corticated two bone fragments above odontoid process, distal clivus is normal.
3.3 Os odontoideum
Odontoid process develops from first spinal sclerotomal except for the os terminale.
Most authors believe that it represents an acquired condition secondary to trauma early childhood [17][18].
Os odontoideum is smooth,
well corticated bone.
Os odontoideum is smaller than normal odontoid and is usually surrounded by hypertrophic atlas anterior arch.
Os odontoideum can make pseudo-joints with atlas [19][16]. Fig. 18 Fig. 19
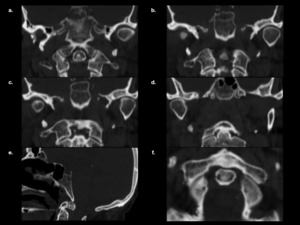
Fig. 18: Os odontoideum: (a.-b.-c.-d.) Coronal reformatted CT image; (b.) Coronal reformatted image, (e.) Mid sagittal reformatted image, (f.) Axial CT image; oval shaped, well corticated bone and hypertrophied and rounded anterior arch of the C1(Atlas).
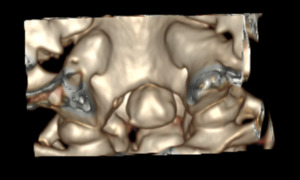
Fig. 19: Os odontoideum: 3D volume rendering image posterior oblique view
3.4 Klippel-Feil anomaly
This anomaly was described by Maurice Klippel and Andre Feil in 1912 [20].
This anomaly is caused by a dissociation defect of spinal sclerotomes in embryological life.
This anomaly is local,
multiple or diffuse in the cervical vertebrae.
The localized form is most commonly seen as a C2-C3 and C5-C6 vertebra fusion.
Segmentation anomalies may be accompanied by basilar invagination,
odontoid hypoplasia,
atlanto-occipital assimilation,
platybasia [3][6]. Fig. 20 Fig. 21 Fig. 22

Fig. 20: Klippel-Feil Anomaly: (a.) Sagittal T2W MR image, (b.) Sagittal T1 MR image; The C6-C7-T1 vertebrae are Partially fusion of the anterior corpuses. (c.) Coronal T2W MR image; Rudimental intervertebral discs are seen at C6-C7 and C7-T1 levels.
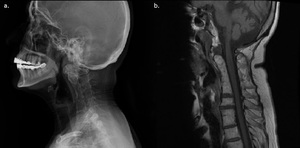
Fig. 21: Complete Cervical Fusion: (a.) Plain Radiography, (b.) Sagittal T1 MR image: The C2-C7 vertebrae are completely fusion of the anterior corpuses. At the same level, the vertebrae are partially fusion of posterior corpuses.
Fig. 22: Aplasia of the atlas and Klippel-Feil Anomaly: (a.) Coronal reformatted CT image; Axis(C2) articulates with hypoplastic occipital condyles. (b.) Coronal reformatted CT image; Right occipital condyle is more hypoplastic than left one. In the Axis(C2) anterior mass, the dens are fused and hypoplastic (c.) Coronal reformatted CT image; C2 left posterior arch aplasictic and C3 posterior arch rachischisis (d.) Volume rendering 3D images; Condylar Hypoplasia, Aplasia of the atlas(C1), C2 and C3 fusion, C2-C3 posterior arch rachischisis.

 Mid-sagittal reformatted CT image evaluated with Welcher basal angle (It is meaningful in terms of platybasia above 140 °). (b.) Sagittal T2W MR image; flattened skull base, enlarged Welcher basal angle. (c.) Volume rendering 3D image; nasion-tuberculum sellae line and tuberculum sellae-clivus line (Tuberculum sellae-basion). (d.) Mid-sagittal reformatted CT image; basilar invagination.")
 Coronal reformatted cervical CT image, red arrows point to clivus. (b.) Coronal reformatted cervical CT image, yellow arrows point to condyles. (c.) Mid-sagittal reformatted brain CT image; flattened skull base, enlarged Welcher basal angle. (d.) Left lateral sagittal reformatted brain CT image; very distinct condyle hypoplasia green arrow point to left occipital condyle. (e.) Mid-sagittal reformatted brain CT image; clivus is almost never developed.")
 Mid-sagittal reformatted brain CT image, (b.) Mid-sagittal T2W MR image; odontoid process above 17 mm on the Chamberlain line. (Basilar invagination) (c.) Mid-sagittal reformatted brain CT image, (d.) Mid-sagittal T2W MR image; clivus canal angle narrowed and spinal canal stenosis.")
 Mid sagittal T2 FLAIR MR image, (b.) Coronal reformatted brain CT image of the same patient, widening of the atlanto-occipital joint axis angle. The complaint from the patient was headache. Hydrocephalus was detected at imaging and clinically confirmed.")
 Mid-sagittal reformatted brain CT images;Condylar hypoplasia and increased anterior atlanto-dental interval, horizontal distance between the anterior arch of the atlas and the dens of the axis, atlanto-axial dislocation is defined as AADI greater than 3 mm in adults. (c.) Mid sagittal T2W MR image; clivus-canal angle is abnormal. Narrowed clivus canal angle should be stimulating in terms of condylar hypoplasia. (d.) Coronal T1W MR image; widening of the atlanto-occipital joint axis angle.")
 Axial cervical CT image (b.) Midsagittal reformatted cervical CT image (c.) Coronal reformatted cervical CT image. Green arrow:C1(Atlas), Purple arrow: Odontoid process, Red arrow: Condylus Tertius. Proatlas persists or fails to integrate clivus, an ossified well corticated remnant present at the distal end of the clivus. (d.) 3D volume rendering image posterior view")
 Mid sagittal reformatted brain CT image; basilar invagination. (b.) Mid sagittal CT image; clivus canal angle is abnormal and angulated odontoid process. (c.) Coronal reformatted CT image; no junction between occiput and atlas, atlas assimilation. (d.) İncreased atlanto-dental interval; Atlanto-axial dislocation. (e.) Volume rendering 3D image; anterior and posterior view.")
 Sagittal T2W cervical MR represents assimilated bone narrow. (b.) Mid sagittal reformatted CT image: mild narrowed clivus canal angle and angulated odontoid process. (c.) Axial CT image, no joint between occiput and atlas; atlas assimilation. (d.) Coronal reformatted CT image, increased atlanto-dental interval; atlanto-axial dislocation.")
 Coronal reformatted CT images; 1.Rudimental left lateral mass of atlas articulates with hypoplastic occipital condyle. 2.Left transverse process of Atlas(C1) is present but right transverse process is not. 3.Atlas(C1) right posterior arch aplasia. 4.Atlas(C1) Posterior arch rashishizis. (b.) Mid sagittal reformatted CT image; basilar invagination. (c.) 3D volume rendering images; 1.Left oblique 2.Posterior 3.Rigth oblique")
 Serial axial CT images of atlas (C1); posterior arch rachischisis. (b.) Volume rendering 3D image; posterior oblique and inferior images demonstrates posterior arch rachischisis.")
 Axial CT image; anterior arch rachischisis. (b.) Volume rendering 3D image; inferior view of split atlas. (c.) Volume rendering 3D image; anterior view of split atlas. (d.) Axial CT image; posterior arch rachischisis.")
 Sagittal T2W MR image; enlarged clivus canal angle. (b.) Axial CT image; represents hypoplastic dens bicornuate. (c.) Coronal reformatted CT image; Platybasia. (d.) Mid sagittal reformatted CT image; hypoplastic dens bicornuate is a very rare malformation. (White arrows hypoplastic dens bicornuate)(e.) 3D volume rendering image; posterior oblique view")
 Axial CT image(yellow arrow); (b.) Coronal reformatted CT image(yellow arrow); (c.) Mid sagittal reformatted image(yellow arrow) (d.) Volume rendering 3D image(red arrows) posterior view; well-corticated two bone fragments above odontoid process, distal clivus is normal.")
 Coronal reformatted CT image; (b.) Coronal reformatted image, (e.) Mid sagittal reformatted image, (f.) Axial CT image; oval shaped, well corticated bone and hypertrophied and rounded anterior arch of the C1(Atlas).")

 Sagittal T2W MR image, (b.) Sagittal T1 MR image; The C6-C7-T1 vertebrae are Partially fusion of the anterior corpuses. (c.) Coronal T2W MR image; Rudimental intervertebral discs are seen at C6-C7 and C7-T1 levels.")
 Plain Radiography, (b.) Sagittal T1 MR image: The C2-C7 vertebrae are completely fusion of the anterior corpuses. At the same level, the vertebrae are partially fusion of posterior corpuses.")
 Coronal reformatted CT image; Axis(C2) articulates with hypoplastic occipital condyles. (b.) Coronal reformatted CT image; Right occipital condyle is more hypoplastic than left one. In the Axis(C2) anterior mass, the dens are fused and hypoplastic (c.) Coronal reformatted CT image; C2 left posterior arch aplasictic and C3 posterior arch rachischisis (d.) Volume rendering 3D images; Condylar Hypoplasia, Aplasia of the atlas(C1), C2 and C3 fusion, C2-C3 posterior arch rachischisis.")
 Sagittal reformatted CT image, (b.) Coronal reformatted CT image, (c.) Mid sagittal T2W MR image (d.) Coronal T2W MR image; N: Nasion, M: Midsellae, T: Tuberculum sellae, Cl: Clivus, B: Basion, OP: Opisthion, HP: Hard palate, O: Occiput, C: Occipytal condyles, C1: Atlas, C2: Axis, D: Dens (Odontoid Process)")